Double checking the claims about Moderna
Data on comorbidities does not undermine previous findings

Steve Kirsch and I have already published our findings on the Czech data showing the lower mortality in the Pfizer population. Our confidence came from four different angles:
The mortality rate was lower for Pfizer in every age group
The mortality rate was lower for every month of injection
The mortality rate was lower for every period of death
It fits with other evidence that Moderna is more pathological
The only way we could have been wrong would be if, in every age group, the Moderna product was specifically given to sick people.
The Czech government have been more transparent with their data recently then any other government. From the recesses of the Czech government’s websites a dataset was found that allowed the claim to be made that sick people were indeed more likely to be given Moderna.
Here is a summary of that data:

Figure 1: Percentage of recipients marked as chronically ill produced by @UncleJo46902375
There are three issues with this data:
It was already known that and Moderna were given disproportionately to the old and there is no accounting for age her
It is being used to claim that a doubling in chronic illness explains a higher rate of death in the Moderna group compared to Pfizer, but another doubling in AZ compared to Moderna there was minimal difference in mortality (see graph in previous post).
It turns out that the column that was being analysed had been mistranslated. It was not the number of chronically ill but "individuals preferentially vaccinated due to chronic disease".
The last point is worth spending a moment on. It is a tick box for an eligibility criteria for vaccination. If it were a measure of chronic disease it should be higher for every age group.
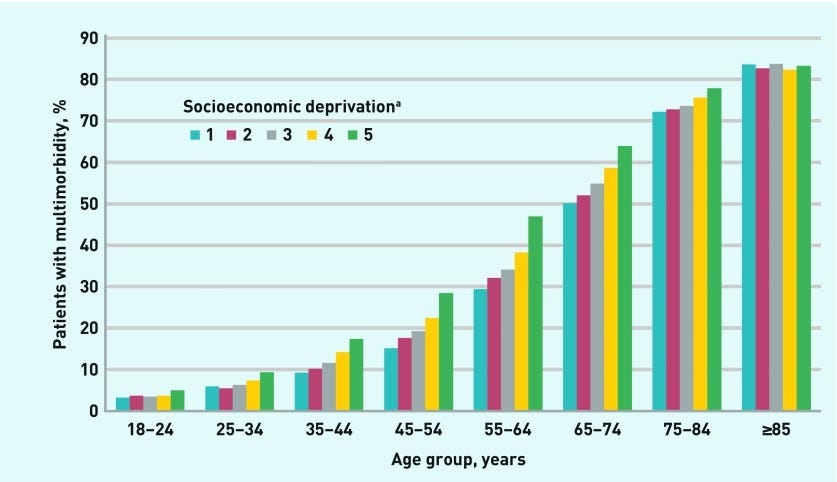
Figure 2: Percentage of population with more than one comorbidity by age in the UK
The Czech data for people vaccinated because of cormobidities looks like this.

Figure 3: Percentage of people who were vaccinated because of any comorbidity
Not only is the fraction of the population who were vaccinated because of a comorbidity far too low to be representative of the total comorbidity in the population but it also tails off with age. Perhaps it was not felt to be important to record such issues in a population where almost everyone has comorbidities and where they were already eligible on the basis of age alone.
There are therefore reasons to be cautious when using this data. However, there was still a problem. It was still true that people vaccinated because of comorbidity were least common among the Pfizer group. Perhaps this was because sick people were more likely to be injected at a GP or hospital where different drugs were available compared to mass vaccination centres? Perhaps it was more to do with how data was recorded in mass vaccination centres compared to elsewhere. I do not know. It has also been suggested that some used this criteria to queue jump.
For a day I toyed with the idea that Steve and I had got this wrong somehow. I was not sure how (given the four points above). It is always harder to be dispassionate about data when you have publicly declared a position already - but I did my best to be. Ultimately, this data does not in any way undermine the point that the mortality rate is far too high in the Moderna, AstraZeneca and Johnson & Johnson groups compared to Pfizer.
The key way to show this is looking at the difference between the period when sick were injected compared to healthy. For 30-39 year olds this is easy as peak vaccinations in the sick were a month before peak vaccinations in the healthy. For other age groups they coincided but we can look at the earlier and later parts of the year instead.
30-39 year olds
I had already attempted to account for this by showing that the date of injection did not affect the difference in mortality rates. However, we could now back that up with data because we could see when the unhealthy were injected. The 30-39 year age group had peak first doses for those with comorbidities in May and peak first doses for the healthy in June. The vaccination rate was high enough in those periods that the number of deaths is just large enough to draw conclusions from. Here are the numbers vaccinated, vaccinated due to comorbidity and dead within a year.

Figure 4: Total people vaccinated, number vaccinated because of comorbidity and total deaths in 30-39 year olds vaccinated with Pfizer or Moderna each month in 2021

Figure 5: Percentage vaccinated because of a comorbidity, mortality rates and ratio of mortality rates for May and June for 30-39 year olds
May saw a peak in the proportion who were vaccinated because of a comorbidity. The percentage with a comorbidity was more than double in the Moderna group and the mortality rate was similarly higher. However, in June the healthy were vaccinated. Again the mortality rate was higher in the Moderna group. More importantly the mortality rate when the Moderna group had 1.7% who were sick was 30% higher (55/42) than when Pfizer was given to a group where 7.2% had a comorbidity. The mortality rate was higher during the healthy vaccination month with Moderna than during the sick vaccination month with Pfizer.
Between 83% and 96% of the sick were injected by May. Comparing the first 5 months of the year with the last 7 months gives us a mortality rate for a period with a high proportion of sick to compare to a period with a low proportion. Picking a later cut off results in a lower proportion with comorbidities and makes it less comparable to the Pfizer data.

The total deaths for AstraZeneca were only ten and the Jan-May ratio is not statistically significant. However, the others all are.
The mortality rate remains higher for non-Pfizer products when both sick and healthy were injected.
40-49 year olds
Again the mortality is consistently higher in the non-Pfizer groups. From Jan-May 4.4% of the Pfizer vaccinated had comorbidities but the mortality rate was higher in the other products from June-December when they had a comparable or lower proportion with comorbidities.

50-59 year olds
The year long mortality rate for those injected in the second half of the year is higher for all vaccine types. This is highly suggestive that those targetted after the bulk had been injected were more likely to have health problems. Other datasets similarly show a markedly high mortality rate in those vaccinated before and after the main period of vaccination for an age group. It is quite suspicious therefore that the records claim only a tiny fraction of these people had comorbidities recorded.
The non-Pfizer mortality rate was higher even when comparing periods with a similar or lower proportion of sick people. Notably the highest mortality for AZ and J&J was when the smallest proportion were recorded as having comorbidities.

60-69 year olds
Similarly, the highest mortality was seen in those vaccinated late for every product. There is little relation between the percentage recorded as having comorbidities and the subsequent mortality rate.

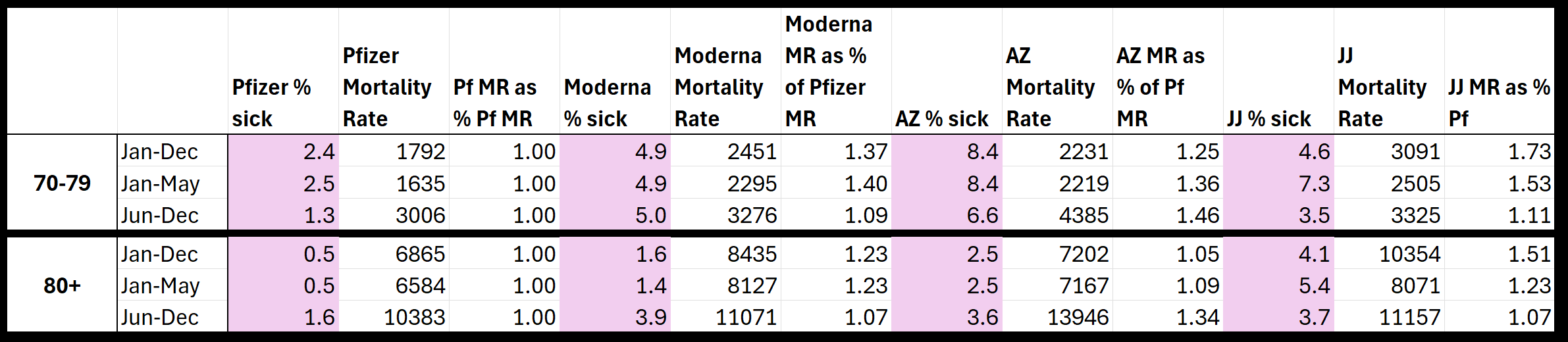
70+ year olds
Again, the highest mortality rate including deaths a year from first injection was seen in the second half of the year for all products. There is no relationship between the percentage recorded as having a comorbidity and the subsequent mortality rate.
Conclusion
Ultimately, the data on comorbidities is unreliable because:
The over 75 year olds have a lower percentage with comorbidities recorded than the under 30s.
Periods where high sickness rates were recorded do not correlate with subsequent high mortality
In the second half of the year, where there was high subsequent mortality, the numbers recorded as having a comorbidity were suspiciously low
Superficially there were differences in comorbidities that might have explained the higher mortality rates in non-Pfizer products but there appears to be inconsistency in how this information was recorded and no correlation between groups with high rates of sickness and their subsequent mortality.
As I have said so many times before, we should not lose sight of who has the burden of proof. Those who brought this intervention have absolute obligation to prove they are both safe and effective to acceptable standards (i.e. at least 95% confidence, 99% in the case of some medical interventions). The fact that we can actually prove the opposite (that they are both unsafe and ineffective), in spite of their feeble attempts to rubbish our analyses, demonstrates how impossible it is for this product to remain on the market for so long, let alone be funded with public money and even mandated in some circumstances. It is blatantly criminal. anyone still buying this BS needs to be in a lunatic asylum or jail.
Imo they're all deadly, some more deadly than others. God help us if this injectable / sprayable / self-replicating / shedding contaminating goopy junk is the future of pharma / politico 'healthcare' for humans and food chain livestock. I hope the wildlife run for the hills (where aerial spraying will get them anyways) 😕