Why I am backing Steve Kirsch on the Czech data
The attackers are wrong

Steve Kirsch cares passionately about the covid vaccines and does not mince his words when he calls out every possible issue. I have been much more cautious about what I have been willing to put forward as evidence of vaccine harm. On the Czech data he is right, I am backing him and here is why.
The claim is that those vaccinated with Pfizer can act as a control group and show that those given other brands had too many deaths. The counter arguments to that claim can be discounted as follows:
1. The unvaccinated died more
Yes, this is true. In fact over the course of the year the vaccinated groups had 40-60% of the expected mortality. Half of the expected deaths did not happen in those groups. That is not because the vaccine was an elixir of life - they clearly weren’t. The expected deaths still happened but they happened in the unvaccinated population. The vaccinated populations are in no way representative of baseline populations because of this. It is totally disingenuous to claim the unvaccinated should have a baseline mortality rate and that the lower mortality rate in the vaccinated is because of the vaccines.
Here is a graph of age standardised mortality. That means the mortality rate for each age group has been mapped to an imaginary population with a set number in each age group and then an overall mortality rate is calculated.

Figure 1: Age standardised mortality rates by vaccination status in the Czech population
There are several important points to make about this graph:
The Pfizer mortality rate (blue) is lower than for other vaccines throughout the period
The difference between Pfizer (blue) and Moderna (red) is similar in July-October 2021 when there were almost no covid deaths to the period before and after when tehre were.
The unvaccinated mortality rate falls over time (compare summer levels) as the dying, who decided not to get vaccinated, die and leave an increasing proportion of healthy unvaccinated behind.
While the unvaccinated mortality rate falls the mortality rate in the vaccinated climbs. We might expect unvaccinated mortality to be higher than baseline in 2022 because the vaccinated were healthier but it should be counter balanced by there being fewer deaths in the vaccinated - as there are with the Pfizer group. However, for all products except Pfizer the mortality is HIGHER than the 2020 baseline by summer 2022.
2. A difference in vaccine efficacy explains the death difference
The consistent difference in months with and without covid means this was not about efficacy. The similar difference in the young and old also makes this impossible.
3. Non-random allocation of vaccines
The main remaining argument is that the products were given out in a biased way i.e. that those more likely to die were given non-Pfizer products.
Let’s imagine a scenario where there was a policy to give ill people Moderna. What would be expect to see if we looked at which age groups received which vaccine. If we looked across the age groups we would expect proportionally more Moderna to be given to 60 year olds than 20 year olds. Yet the proportion of Pfizer was equal across these age groups at between 91-93% of doses. In older age groups slightly more Moderna was given. Because of this we analysed 20-69 year olds first and then verified with older age groups.

Figure 2: Pfizer doses as percentage of total doses given by age group
Perhaps it wasn’t about illness as such and more about markers for illness such as socioeconomic deprivation. Imagine there were regions within Czechia which were poorer and they were given Moderna. The trouble with this is that the age demographic for these hypothetical regions is an exact match for the population as a whole which seems highly unlikely to me.
4. All the other evidence
People denying this evidence are not facing up to the myriad of other evidence that points to the same conclusion.
The dose of Moderna is three times the dose of Pfizer. Pfizer rejected a higher dose because of toxicity in the pre-clinical trials.
The Fraiman paper on the clinical trials showed 10 excess serious adverse events of special interest per 10,000 doses in the Pfizer trial but 15 for Moderna.
The adverse event reporting systems had more reports for Moderna than for Pfizer in every country.
Finally, one important take away for me is that in England and Wales we saw a notably higher mortality rate among people under 64 than those over 64 after the rollout. I had always put this down to a deaht deficit in the old coming after a period of high mortality. However, perhaps the different products given to different age groups is an important point too.
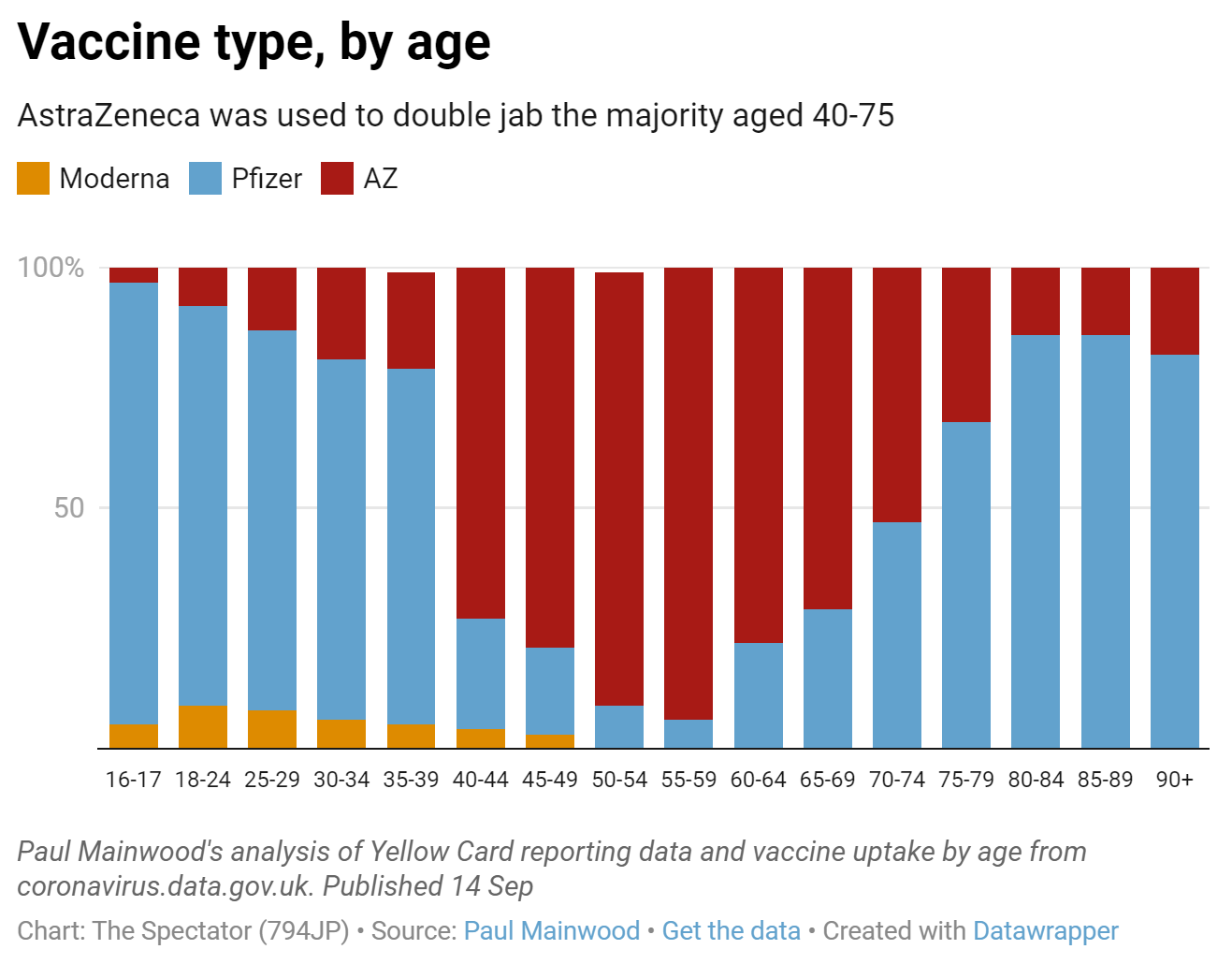
Figure 3: Vaccine type given by age in UK from Spectator Data Hub
Steve has written in much more detail countering these claims on his newsletter here, and here, but this is a big picture overview of the major issues. I am still working on the evidence for how much of a mortality risk each product presented.
Thanks Dr. Craig! I have been following Steve Kirsch, but because I am not able to really understand the data very well (I had Biostatistics in the School of Public Health at UCLA 47 years ago 😂😩)I have been waiting for someone highly credentialed to weigh in. I also enjoy your conversations and insights on Dr. Campbell’s You Tube channel. I do hope other highly credentialed scientists offer their opinions as well.
As a patholgist, I urge you to read Frances Leader's article on those white fibrous clots being found. There is a link to a video which is now restricted. Frances added some screen shots of the video which shows what it is, what it's doing and how they already knew this would happen as several studies prior to 2020 showed this. francesleader.substack.com/p/white-fibrous-clots Thankyou.